How can Dutch Corona policy, and the broader Great Barrington Declaration thinking, be well-intentioned and make the cabinet proud, but also be considered a crime by many?
When a report was published on 14 October 2021 that concluded that the Netherlands chose the wrong Corona strategy, D66 (liberal party supporting the caretaker Government) MP Jan Paternotte reacted in relaxed way that we should consult better with our neighboring countries next time. Cabinet members are proud of the policy they pursued. But for many people, the Dutch strategy is morally wrong; the WHO even called it "unethical" and an Amsterdam scientist went even further with the word "eugenics".
How can the same Corona policy be a good thing and a crime? The answer lies in the logic of the influenza playbook. Until we all understand that logic, people who assume the best intentions from the government will not be able to accept that the Netherlands had and has a policy of as many infections as possible, no matter how much the facts show this to be true. But good intentions do not save a country from disaster. And bad intentions are not necessary for a policy of "controlled rampage" of a deadly virus.
With the lifting of almost all measures under high virus circulation, the Netherlands entered a new pandemic phase. Everything points to people hoping to be able to leave not only the disease, chaos and confusion behind them. but also discussion about policy choices. It is natural to want to look ahead after a traumatic period. But the problem is that the trauma is far from over, and there is a lot of mistrust, anger and even violence. That trauma will not pass if we do not name, understand and evaluate the chosen and still very much operational corona strategy. Not as an evil “eugenics” or simplistically “corona dictatorship”, but as an understandable political and moral choice. Which was, however, never a good plan and from which the country must be liberated.
This article is written by Michael Blok and appeared on October 21st, 2021 in Dutch, and was subsequently published in English on November 14th, 2021.
The Netherlands lets it sink in: we did and do things differently
Europe and North America decided in early 2020 that the virus could not be stopped, or at least not immediately. And if it could be stopped, it would always come back from abroad anyway (from which foreign country has never become clear, since most of the rest of the world contained the virus quite diligently). Most Western countries therefore did not take the measures that would have been necessary to get rid of the virus, which is why, according to a WHO report, they did not succeed. The infections had to be slowed down considerably to gain time and to keep health care accessible, was the idea. The alternative was to allow an unchecked rampage of the virus, resulting in countless deaths among Covid patients but also others who would no longer be able to receive health care.
But the Netherlands went a step further. In March 2020, it became the only country in the world to officially announce the strategy of “maximum control”. This approach, called "controlled rampage" within government circles, tried to shield the elderly and prevent excessive burdens upon the health care system, but otherwise to let the virus circulate as much as possible. Because people who survive the infection become less contagious, the outbreak would lose its momentum and normal life could resume soon. Because an overload of care is inevitable, and then brakes again, the cycle of yo-yo lockdowns that RIVM CEO Jaap van Dissel had also announced at the beginning of 2020. Up and down, amassing immunity as quickly as possible.
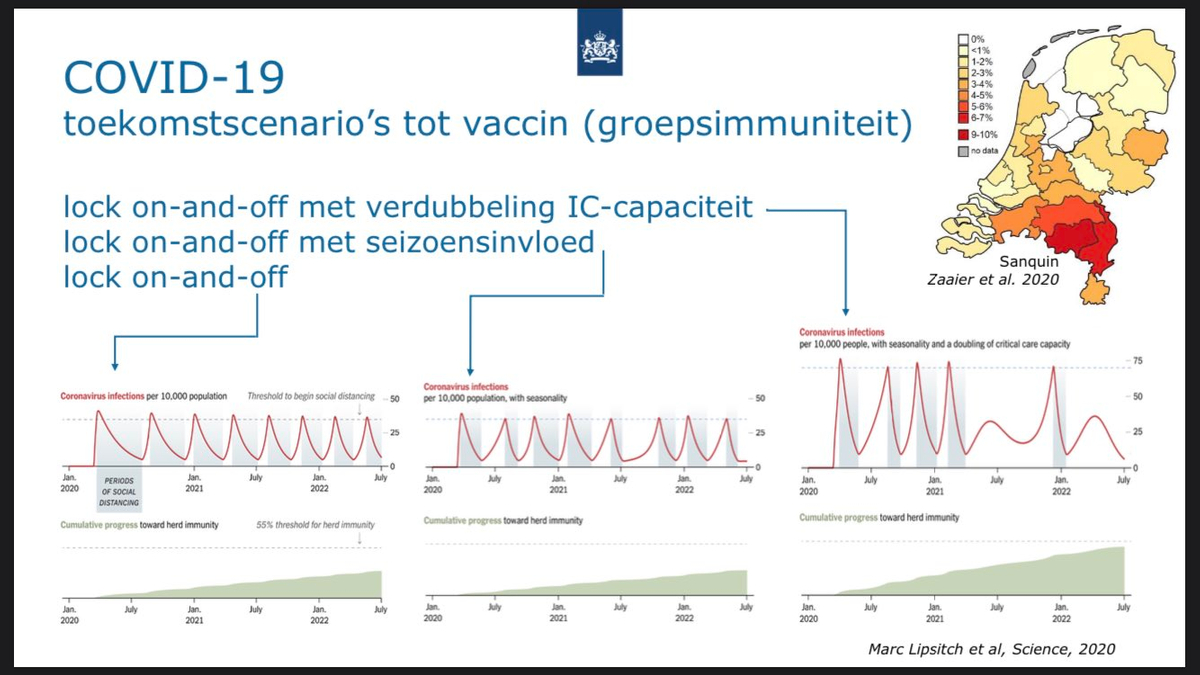
Slide from van Dissel's presentation, showing recurrent (semi-)lockdowns and the result of an antibody study
This strategy has not been successful. The "vulnerable" often died because of a lot of virus. The healthcare sector has been under severe pressure for a year and a half and now also sees a large exodus of nurses and doctors. Because the Netherlands braked late and weakly (to amass more immunity), the Netherlands has had a relatively large amount of control measures. The social fabric has been damaged by the unclear and incorrect communication from the government. The many infections with this vicious virus have led to hundreds of thousands of long-term sick people, far more than in countries that curbed the virus harder and faster and gave almost everyone a chance to vaccinate before they became infected. And there is now an atmosphere of tension, anger and fatigue in the Netherlands, while countries that went for little virus are proud of the solidarity and successes achieved. Tensions and violence that we predicted in the Spring of 2020, because they were not difficult to predict by those who understood the government's plans.
Policies that are unsuccessful, and still very much alive, are normally debated. In the Netherlands it seems rather taboo to look back. When BIJ1 (anti-racist left party) MP Sylvana Simons held the cabinet responsible for the high Covid mortality in our country in a parliamentary motion, outgoing Prime Minister Mark Rutte reacted as if stung by a wasp. 149 MPs did not join the motion, although an almost identical earlier motion received broad support.
When University of Amsterdam lecturer Matt Cornell gave an excellent motivation for his resignation and emigration from the Netherlands, many people took offense at the word “eugenics”. But the introduction of the QR code (green pass) in the catering industry is also experienced as “dictatorship” and “exclusion” by many people. Many even wear Jewish stars in protest. Both camps feel deeply morally offended.
How can the same policy be immoral because it's too flimsy, but also because it's too strict? How can the cabinet be proud of “more infections than Germany and Denmark” when such a policy is considered “unethical” by the WHO and simply led to more unnecessary deaths? In order to understand that, we need to understand how the ministers and officials who devised and implement the unique Dutch policy think about this epidemic. And that analysis starts and ends with the Flu Playbook.
Herd immunity as a wise choice
"it's a bad flu!"
At the beginning of 2020, all of Europe thought that the virus, just like previous "Chinese" viruses, would blow over. But we also agreed that stopping the virus would not be possible if it got a foothold. The Netherlands therefore based its policy on the playbook for the "closest" disease: the flu.
Every country is affected by one or more flu waves every year. This disease is risky, and if too many people become infected, hospitals are occasionally overloaded, and in extreme scenarios even power production can fall prey to mass sickness. The aim of the government is to prevent this, of course. The easiest way to prevent chaos in hospitals is to ensure that infections mainly affect the young, making them immune, and that the number of infections then falls due to herd immunity when it becomes safer again for the most vulnerable people to go out. In addition, it is very important for the economy that people do not become afraid of getting sick, because then people will sit at home for months without producing anything. They will get sick anyway, many of the healthy working people, so waiting is just a waste of time and money.
The models that RIVM (Dutch CDC) uses for policy making are based on the assumption that people who have been infected can no longer infect, and if they survive the disease, they will no longer be hospitalized. This can make containment and keeping infections low seem unattractive.
Many factors contributed to the Dutch choice to go for a herd immunity sprint. The first thing to consider is the fact that most of the Western world decided to not try to stop the virus, but merely to slow the spread and buy time for a vaccine. That choice, which in itself was not a wise one, was based on a number of contributing factors:
- Experiences of Asian-originated viruses never making it to Europe
- When such viruses made it to Europe, they were often contained or didn't cause too much trouble
- A lack of means to combat outbreaks (personnel, IT, masks)
- A sense of cultural superiority or, more charitably, a sense of invulnerability after a Century of lack of an outbreak that caused much harm to (heterosexual) Europeans.
But the Netherlands, along with Sweden and the UK, went much further than other European countries. The following elements certainly contributed to this choice:
- Cost effectiveness thinking (see below)
- Tolerance for disease and the chickenpox party philosophy (see below)
- Lack of experience in containing pandemics (although the Netherlands is very good at containing MRSA)
- A right-wing government that takes business-friendliness to extremes (viz Boris Johnson's "red cape flowing")
- A clubby small country with extreme trust in government (making a rampage sellable with compliant media)
- Outbreak control combining power, information, advice and communication in one person (Prof. Jaap van Dissel)
It is no coincidence that the above elements also apply to Sweden, Switzerland, Belgium and England, which all also chose a herd immunity strategy to some extent.
Cost effectiveness thinking
The Netherlands is one of the few countries where cost-effectiveness is used for decisions about medical treatments. This means that a treatment will often be stopped (or never started) if it does not "pay for itself" in terms of cost. This means that if someone gains 10 healthy years of life thanks to a treatment for a serious illness and the treatment costs less than 800,000 euros, the patient will be treated. These life years are adjusted for "quality of life", whereby, for example, being in a coma gives very little life value: the Quality Adjusted Life Years. But also being in a wheelchair or otherwise handicapped "costs points". And so old people, but also people who continue to have health problems after illness and treatment, are less likely to be treated for a condition than healthy young people.
This QALY-thinking is an ethically very complex issue, which is both scientifically controversial and tacitly accepted in Dutch society. It reduces complex considerations to money. It makes the life of someone with pain or a disability less valuable, while there is nothing objectively meaningful to say about that. It implies that people's lives do not all have the same value, which is very sensitive in, for example, the German moral and legal framework. All these reasons for most countries to organize health care considerations more flexibly than the Netherlands and, for example, Sweden and the UK also do.
In this pandemic, QALY thinking contributes to the fact that the government gives the virus a lot of room. In early 2020, based on the models at the Ministry of Health, it seemed that a lockdown would cost much more than it would yield. The logic is that lockdowns are bad for the economy, but also that slowing down and delaying Covid infections would crowd out other health care, which in turn would lead to more deaths. These calculations were wrong, because it's not not measures that cost money and make people sick, but the virus. The models yield an end point which does not exist and underestimate the value of track, trace and isolate systems and the opportunity to contain the outbreak. Countries that quickly curbed the infections have on average gotten through 2020 and 2021 better. But what matters for this analysis is that the mathematicians who wanted a lot of virus were not of ill will: the intention was to protect society by tolerating a lot of virus.
The chickenpox party
As with chickenpox, the establishment's idea seems to be that an infection at a young age is a kind of gift. This gives a a person the chance to build up resistance at the age that it causes the least damage. The former top adviser to British Prime Minister Johnson revealed that there was literally talk of a "chickenpox party" as the strategy: get the children immune quick, better for the economy, better for the elderly but also for the children themselves. This thinking could explain why government-linked pediatricians in the Netherlands have actually been spouting talking points on TV for a year and a half with the only effect of infecting children as soon as possible with an unknown and certainly not risk-free virus. Politically logical, but not an obvious act for a doctor.
In summary, the virus needs to be rushed through the young population quickly. The expected mortality is seen as “written off” and anything that can be saved on the total mortality (by quickly infecting young people and avoiding the elderly) is successful government policy. The caretaker cabinet Rutte is proud to have saved lives, which Minister Ferd Grapperhaus also indicated by talking about "well-dosed lockdowns" through which the Netherlands had achieved more natural infection and "lower mortality than other countries" (which is very much untrue, that latter bit).
When you're saving lives and the economy in the biggest crisis in most people's memory, necessary lies are obviously a minister's duty. In the case of the flu, this is limited to the prevention of large-scale fear of infection. But with the much more dangerous and contagious Covid, more was needed. And that is why RIVM director Van Dissel changed course at the end of January 2020. Where he previously spoke about contamination through inhalation/aerosols and the importance of masks, he turned around to contamination by spatters and the false safety of masks. He invited people to go to Carnival “because it is celebrated in small groups”. RIVM and the cabinet then came up with a lot more incorrect communication, such as "children play no role in the spread", "masks do not work well" and "the Delta variant is a bit more contagious".
And so well-meaning politicians arrive at a policy that targets many infections. But a large part of the world (scientific and political) thinks otherwise. When you talk about this with Dutch medical insiders, or listen to the TV, they say things like:
- Other countries also want to build up herd immunity through the children, but do not dare to do so for legal reasons (prosecution for culpable homicide, as is already happening in Spain and France).
- Our care is the best, we know better
- Only in a country like the Netherlands is the control necessary to rage without chaos possible.
The other angle: Herd immunity as a crime
But people who do not see total death from an epidemic as inevitable, with a public health attitude, turn that reasoning around. Then everyone who dies is a loss, and preventing infection is gaining time. At Containment Now, it took a while in March and April 2020 for the simple logic of government policy to sink in, because from the thinking of most of the world it is very strange to aim for many infections with a deadly virus (among the healthy, at least). .
Proponents of herd immunity say that those people will die anyway: why do we all lock ourselves up for years if we get infected afterwards anyway? That reasoning sounds good, but forgets the value of gaining time. As months go by, the treatment gets better, so getting sick later is better. And most importantly, of course, the pharmaceutical industry surprised the world by coming up with excellent vaccines in just a few months. Mortality can now be largely prevented. In fact, the herd immunity sprint in the Netherlands has been a gamble that vaccines would take years to come, or that it would be too expensive to wait 9-12 months. Both turned out not to be true.
And so, countries such as Denmark, Norway or Finland have a good chance of surviving the pandemic without serious Covid deaths. If a country such as the Netherlands, which circulated the virus a lot based on flu thinking, has a high mortality rate, that mortality can no longer be dismissed as "inevitable total mortality". A recent report from KMPG confirms that the Netherlands has actually lost some 25,000 unnecessary lives. When people die who don't have to die, that's not acceptable.
It even seems that vaccines inhibit infections, at least temporarily. Countries where the virus was contained early and strictly, where authorities always communicated clearly and openly, and where vaccination was lightning fast, it seems that for the time being it is possible to make do almost without painful control measures. For the Netherlands, that is still a distant dream. A third shot, or the highly effective second shot in people who received Janssen, is not being considered by the government. The logic still seems to be that the virus is harmless to "normal" people, especially if they are vaccinated. They may also benefit from a "booster" infection. That is not the case, but above all, the (temporary) inhibitory value of vaccination remains unused. Because remember: not a little, but a lot of infections is the basic instinct.
Also, the choice to let infections mainly pass through the young, if that infection is not inevitable, is not a gift to those children, but harm. In a sense, the government claims the bodies of, for example, school children for a societal purpose. This is, of course, morally and legally unforgivable. Especially because we know from release FIA documents that the central government knew at the beginning of 2020 that children get less sick from Covid, but not how sick. And now there are vaccines, including for children. As the German Ethical Council ruled, just forcing the virus upon our young is not ethical, and even less so when it's under threat of removal from parents, as in the Netherlands.
The risk has been deliberately taken that young people are indeed vulnerable, and it shows. Covid death among young people is rare, but long-term illness is common. The risks of Covid are close to those of measles or polio, and we don't take those diseases lightly. That is why the WHO, ECDC and most governments are arguing in favor of combating infection in schools. The Netherlands is deliberately letting the virus run free there. A tour of top experts in the US shows that they do not think loosely at all about the contamination of (their) children, so the RIVM (Dutch CDC) is likely to know that there are serious risks. But if the risks are smaller than with the elderly and you try to minimize total pandemic damage in a mathematical model that assumes the pandemic ends when enough susceptible bodies are reached, the schools are given the green light.
There is another way in which Dutch policy can be labeled a crime. Several countries accepted that many people would get Covid before being vaccinated. In general, however, these countries did not allow healthcare to fail. In Germany, Ireland and Italy, for example (except Lombardy, where the first European outbreak occurred), regular care has never come under extreme pressure. In March 2020, the Netherlands saw health care overflow by a factor of 3 or 4, and since then the number of postponed operations has increased in most months: too much Covid, but also too many sick and stressed health care workers. The sector is now openly talking about collapse. This means that death and illness due to the Dutch Corona policy are to a large extent not limited to people who have Covid.
Addicted to infections
Hopium!
The question, of course, is why the Dutch-British-Swedish approach is maintained after the logic and decisions of early of 2020 turned out to be incorrect. Controlling the outbreak for years turned out to be possible in other countries, the economy appeared to thrive more where there was little virus, shielding the elderly proved impossible, durable herd immunity due to infection never happened, and people who become infected often become seriously ill for a long time or even permanently. Covid is not just "pneumonia" but a disease that can affect the body anywhere, often including the brain and heart.
The persistence of a strategy overtaken by the facts will lie in the character of the political leadership, which does not like to change course. But in a procedure-driven country like the Netherlands, don't underestimate the power of the playbook either. Outbreak Management Team member Marc Bonten spoke about an automatic follow-up step of IC-driven mitigation if containment fails upon arrival of the virus. Going back to containment afterwards just isn't in the flu playbook. Not even in New Zealand, for example. But when Prime Minister Ardern tried and succeeded there to put the virus back in its cage, other countries followed suit.
Outgoing Prime Minister Rutte also considered going for low virus levels virus in the late Spring of 2020, but published documents show that he was opposed by RIVM/CDC boss Van Dissel. And so the concentration of power in one person plays a major role: this doctor is the infectious disease director at RIVM, director of the local health authorities, chairman of the OMT and defender of government policy in the House of Representatives. What he wants happens, and what he did he cannot undo without many negative consequences for himself.
And so the Netherlands is on the eve of a new winter of chaos. The OMT calculates that there are still 5,000 ICU admissions that need to pass through the system with Covid, which equates to at least 10,000 additional deaths, tens of thousands of temporary or permanent disabled people with Long Covid and potentially another 1 or 2 years of Covid-filled ICs. The current healthcare collapse could also get even worse. This makes it attractive for the outgoing cabinet to burden the health care sector once again (and relieve the ICU burden by withholding Covid care, the well-known oxygen tank at home, but also informal admission stops from nursing homes). The signs for that are there. If such a new mass infection sprint actually takes place, foreign countries will again impose restrictions on the Dutch (Morocco is already there, and others are following suit although capped testing is making infection levels look artificially low) and at some point a kind of lockdown will be instituted again.
Groundhog Day in the polder.